
Health
How to Understand Legionnaires’ Disease, Which Has Sickened Scores in NYC.
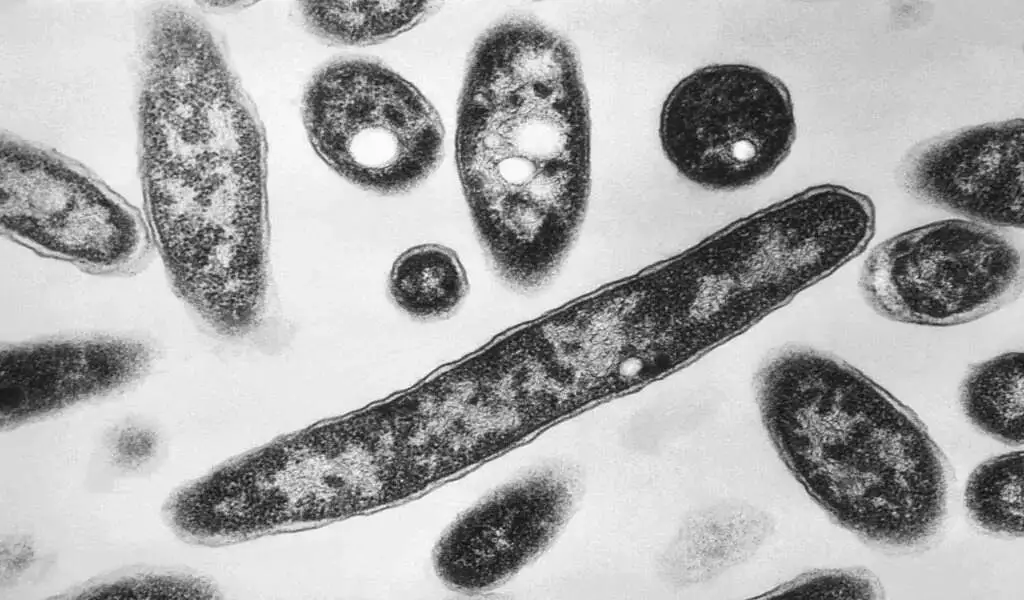
(VOR News) – The outbreak of Legionnaires’ disease in New York City has resulted in the illness of 58 individuals and the mortality of two, as of the end of July.
The outbreak that occurred in Central Harlem has been attributed to cooling towers, which are structures that utilize a fan and water to chill buildings, by the scientists from the city’s health authority.
However, we have resolved the issue. Initially, it was reported that eleven of these structures had tested positive for a specific type of bacteria that is responsible for Legionnaires’ disease.
However, the issue has been resolved.
It was strongly advised that individuals in the vicinity who were experiencing symptoms that were similar to those of the flu contact a medical professional at their earliest convenience.
This was of the uttermost importance to individuals who were fifty years of age or older, had lung diseases that had been present for an extended period of time, or smoked. You are only required to be cognizant of this.
How do you define Legionnaires’ disease?
This specific form of pneumonia is caused by Legionella bacteria. These bacteria have the capacity to proliferate in warm water and can also replicate throughout the water systems of buildings.
In addition to hot springs and showerheads, they may also be present in cooling towers and other comparable devices. It is feasible that you will find them in these locations. One of the most common ways to contract the disease is by inhaling aerosols generated by contaminated drinking water.
In addition, hospital patients may contract the Legionnaires’ Disease by ingesting contaminated ice or drinking water that has been contaminated with the virus, according to public health officials.
Furthermore, infants may be susceptible to the disease if they ingest water that contains the harmful substance. As a result, it is wholly impossible for individuals to acquire it from one another. According to the Centers for Disease Control and Prevention in the United States, symptoms may manifest within two days to two weeks of exposure.
For the majority of patients, this is the moment at which symptoms appeared. This condition has been linked to various symptoms, such as wheezing, fever, headaches, muscle aches, and shortness of breath.
What are the potential therapies for Legionnaires’ disease, in addition to the symptoms and indicators that are associated with this condition? Public health professionals have emphasized the significance of receiving both a diagnosis and treatment with the appropriate antibiotics as soon as feasible.
According to the World Health Organization (WHO), the severity of the illness can deteriorate during the initial week when treatment is not administered. Shock, renal or organ failure, and respiratory system failure are among the potential complications that may develop.
What can one do to prevent Legionnaires’ Disease from occurring?
The World Health Organization (WHO) has stated that the personnel responsible for the safety of water systems and buildings have the capacity to mitigate the risk by instituting measures that will limit the bacterium’s growth.
To illustrate, they should conduct routine cleansing and disinfection of cooling towers, ensure that spa pools are adequately chlorinated, and flush the taps of buildings that are not in use once a week during the week. The following are just a few of the objectives that personnel responsible for water safety should be able to accomplish.
By performing various preventative measures within the confines of their residences, it is feasible for individuals to mitigate their susceptibility to Legionnaires’ disease.
According to the health officials of New York, it is recommended that garden hoses be drained, water filters be cleaned and replaced in accordance with the manufacturer’s instructions, chlorine levels in pools and hot tubs be regularly monitored, and hot water heaters be flushed once or twice annually.
SOURCE: AP
SEE ALSO:
China Reports Thousands of Chikungunya Cases Amid a Mosquito-Borne Outbreak.
The sniffles? Discover How COVID-19, Summer Colds, And More Can Affect You

A new COVID-19 variant known as “Cicada” is drawing quiet attention from health officials across the globe. Its official name is BA.3.2, and this heavily changed strain has turned up in wastewater testing in at least 25 U.S. states.
While COVID levels remain fairly low overall, experts are watching the variant closely because it may be better at slipping past existing immunity.
The nickname fits the story. Much like cicadas that stay hidden underground for years before appearing all at once, BA.3.2 seems to have circulated under the radar for a long time before becoming easier to spot.
Public health leaders say there’s no reason to panic, but staying informed still matters, especially as summer gets closer.
What is the Cicada COVID-19 variant?
Cicada is part of the Omicron family, and more precisely, it belongs to the BA.3.2 sublineage. Scientists first identified it in a respiratory sample collected in South Africa on November 22, 2024.
It carries a striking number of mutations, with about 70 to 75 changes in the spike protein alone. Because of that, it looks quite different from more recent strains that came from the JN.1 family.
Experts describe BA.3.2 as highly mutated and part of a separate branch of the virus. As a result, it stands apart from the variants that have spread most widely in the United States since early 2024.
Biologist T. Ryan Gregory gave it the “Cicada” nickname after noticing how long it stayed mostly out of view, similar to cicadas during their early underground stage. After a slow start, the variant began rising more clearly in September 2025.
Where Has the Cicada Variant Been Found?
So far, BA.3.2 has been detected in at least 23 countries across Africa, Asia, Europe, North America, and Oceania. In the United States, the CDC has confirmed its presence through several types of tracking.
- Wastewater samples from 25 states
- Nasal swabs from international travelers
- Clinical samples from patients
- Airplane wastewater from some flights
The first known U.S. detection came in June 2025 at San Francisco International Airport. It was found in a traveler returning from the Netherlands. Since then, detections have gradually increased, although the variant still makes up only a small share of total sequenced cases.
In parts of Europe, the variant reached roughly 30% of sequences in countries such as Denmark, Germany, and the Netherlands during late 2025. Even so, those increases did not trigger a sharp jump in overall COVID case counts.
Why the Name ‘Cicada,’ and What Sets It Apart?
The nickname makes sense for more than one reason. Cicadas spend years hidden below ground, then emerge in noticeable waves. Similarly, this variant stayed mostly unseen for more than a year before health officials began finding it more often.
Unlike many recent Omicron descendants that came from JN.1 or LP.8.1, BA.3.2 appears to come from a separate path. It traces back to the older BA.3 lineage, which had seen very little circulation for nearly four years.
That long stretch of quiet change gave the virus time to collect many new mutations. Scientists say those changes may help it dodge part of the immune protection built from past infection or vaccination. Still, current data does not show that it causes more severe illness.
Symptoms of the Cicada Variant
So far, the symptoms linked to BA.3.2 look much like those seen with other COVID infections. Health officials have not reported any unusual warning signs or a clearly more dangerous symptom pattern.
Common symptoms include:
- Cough
- Fever or chills
- Sore throat
- Congestion or a runny nose
- Shortness of breath
- Fatigue
- Headache
- Loss of taste or smell (less common now)
- Sneezing
- Muscle aches
Most people who get sick have mild to moderate illness, especially if they’ve been vaccinated or infected before. Still, some groups face a higher chance of complications, including older adults, young children, and people with weakened immune systems.
If you start feeling sick, stay home and test if you can. That simple step can help lower the spread to others.
How Concerned Should People Be About the Spread?
At this point, COVID numbers in the United States remain relatively low. Recent reports show test positivity around 3% to 4%. BA.3.2 accounts for only a small portion of cases, but its appearance in wastewater across many states suggests it may be spreading more widely than case testing alone shows.
Experts say today’s surveillance tools are much better than they were early in the pandemic. Wastewater testing works as an early signal because it can pick up viral spread before many people seek care or take a test.
Travel still matters, too. Many detections have been linked to international travelers arriving from places where the variant became more common earlier.
A summer wave is possible, but no one can say for sure yet. Some countries in Europe saw increases without major stress on hospitals. For now, health agencies are focused on whether BA.3.2 shows any changes in spread or severity.
Vaccine Protection and the Cicada Variant
Current COVID vaccines are designed around antigens from JN.1 and LP.8.1 lineages. Since BA.3.2 has many spike protein changes, experts are concerned that protection against infection may be lower than it is for more closely related strains.
Even so, vaccines still do a strong job of protecting against severe illness, hospitalization, and death. That remains true even when a variant shows some immune escape. Updated 2025 boosters likely still provide at least some cross-protection.
The CDC and WHO continue to urge people to stay up to date on vaccination, especially those at higher risk. Antiviral drugs such as Paxlovid also remain effective against most Omicron-related strains.
Basic steps still help reduce risk:
- Wash your hands often
- Improve airflow in indoor spaces
- Wear a mask in crowded places if you’re at high risk
- Stay home when you’re sick
What Health Officials Are Saying
Dr. Robert H. Hopkins Jr., medical director of the National Foundation for Infectious Diseases, has said the variant stayed mostly undetected for a long period. He also compared its pattern to the insect that inspired the nickname.
CDC researchers say they were able to spot BA.3.2 early because they now use more than one kind of surveillance. That includes genomic sequencing, wastewater tracking, and traveler screening.
The World Health Organization added BA.3.2 to its “variants under monitoring” list in December 2025. Since then, the agency has continued to spread and develop along with other strains.
Infectious disease experts also stress the need for perspective. COVID is now endemic, and new variants appear regularly. Most of them lead to manageable waves rather than the kind of crisis seen in the early years, largely because of vaccines and prior infections.
The Global Picture and What Comes Next
Detections of BA.3.2 are still rising slowly in several regions. In some parts of Europe, the variant briefly reached about 30% of sequenced samples without pushing overall case levels much higher than in past seasons.
Countries in Asia and Africa have also reported cases, which shows how quickly the virus can move across borders.
Scientists are also tracking related offshoots such as BA.3.2.1 and BA.3.2.2. That kind of change is normal for SARS-CoV-2, which keeps mutating as it spreads.
Looking ahead, researchers expect more variants to appear. The main concern is whether a future strain will combine fast spread with more severe illness. So far, Cicada does not seem to fit that pattern.
Summer travel could still shape what happens next. More movement between countries, plus time spent indoors in air-conditioned spaces, can help respiratory viruses spread more easily.
Tips to Stay Safe This Season
You probably don’t need to change your whole routine, but a few practical steps can still make a difference.
- Check your vaccine status. Ask your doctor if an updated shot makes sense for you.
- Test early if symptoms show up. Home tests still help catch active infection.
- Improve indoor air quality. Open windows or use HEPA filters when possible.
- Follow updates from trusted sources, such as the CDC or your local health department.
- Support community protection. Higher vaccination rates help shield people at greatest risk.
If you’re in a high-risk group, taking extra precautions during times of higher spread is a smart move.
The Bigger Picture of COVID Changes
The rise of the Cicada variant is another reminder that the virus keeps changing. Still, communities have adjusted in major ways. Treatments are better, vaccines are widely available, and most people now manage COVID much like they do flu and other seasonal illnesses.
Research into broader coronavirus vaccines may eventually lower the impact of future variants. For now, the best approach is layered protection, which means staying vaccinated and using basic precautions when needed.
Health systems are also better prepared than before. Hospitals keep track of bed use and maintain plans in case cases rise again.
Final Thoughts
The arrival of BA.3.2, also called Cicada, shows why strong surveillance systems still matter. When scientists catch a variant early, they have more time to study it and guide the public.
Although headlines about a new strain can sound alarming, the evidence so far suggests BA.3.2 acts much like recent variants. It may spread well, but it does not appear far more dangerous.
Stay informed, keep sensible habits, and pay attention to updates from trusted health agencies. If cases rise this summer, there are still tools in place to respond. Your local health department and news outlets can also help with advice that fits your area.
Trending News:
RFK Jr Introduces the New Food Pyramid to “Make America Healthy Again”
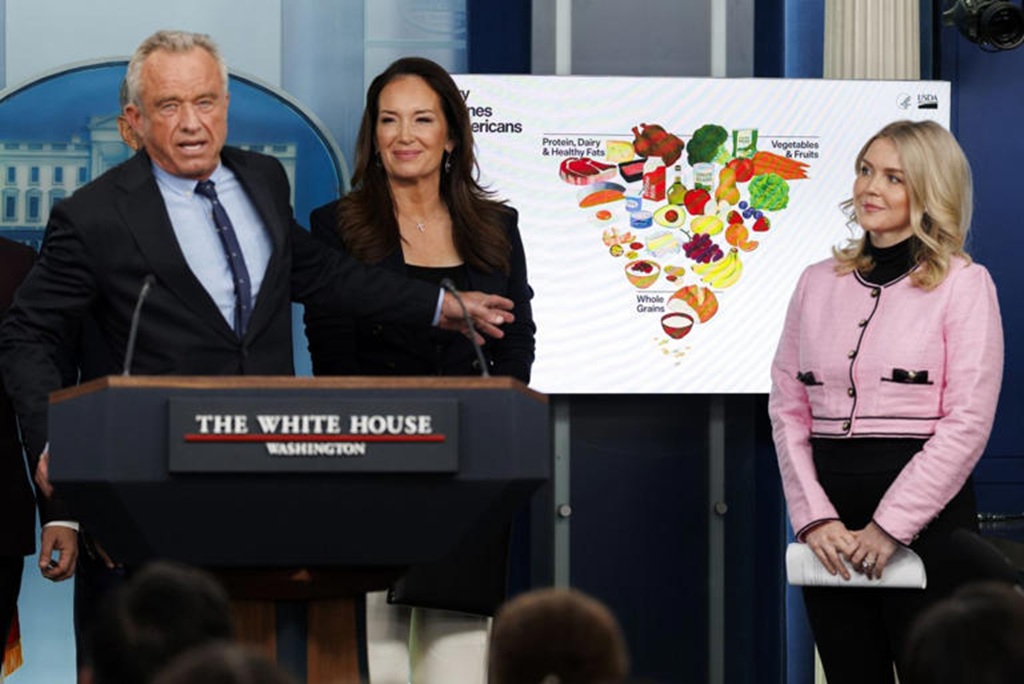
WASHINGTON, D.C. – HHS Secretary Robert F. Kennedy Jr. stepped into a packed briefing room this week to introduce the New Food Pyramid, the “2025-2030 Dietary Guidelines for Americans.” Supporters are calling it the biggest shake-up in federal nutrition advice in decades.
The headline change was hard to miss: a redesigned food pyramid that looks almost flipped. Kennedy didn’t soften his message. He said the old approach helped fuel chronic illness. He also said it’s time to stop treating fat like the enemy and start cracking down on added sugar and ultra-processed foods.
For years, the classic food pyramid, and later the MyPlate graphic, put grains like bread, cereal, and pasta at the base. Fats and oils were pushed to the side with warnings to limit them. The new model reverses that idea.
The broad base of the updated pyramid highlights high-quality proteins and healthy fats. The list includes red meat, eggs, poultry, and full-fat dairy such as whole milk and cheese. Kennedy said these foods were unfairly discouraged for a long time. The guidelines also support cooking with butter and beef tallow, moving away from heavily processed seed oils that became common in American kitchens in the 1990s.
Marty Makary, the FDA head who appeared alongside Kennedy, said schools and parents shouldn’t feel like they have to avoid fat at every turn. He said whole-food fats support brain health and growth.
Food Pyramid Takes a Hard Line on Added Sugar
As protein and fats move to center stage, the space for carbs shrinks. Refined grains, including white bread and crackers, sit at the narrow top of the chart.
The biggest shift is the federal position on sugar. For the first time, the guidance says no amount of added sugar is recommended for a healthy diet, with extra focus on children. The new rules set a limit of 10 grams of added sugar per meal, far lower than past advice.
Kennedy said the government needs to be direct with the public. He blamed added sugar and chemical additives for driving obesity and diabetes rates. He also said the country can’t claim it cares about health while supporting the ingredients that contribute to disease.
What It Means for Schools and SNAP
These guidelines are not just tips for people cooking at home. They shape what federal programs can serve. That includes the National School Lunch Program, which provides meals to about 30 million kids each day. If the guidance holds, school menus will need major updates.
Changes expected in many cafeterias include:
- Whole milk is returning, replacing the fat-free and chocolate options now common
- More main-dish proteins, such as beef and eggs
- An end to sugary fruit drinks and highly processed snack packs
Agriculture Secretary Brooke Rollins, who helped write the report, said the plan is also meant to support American ranchers and farmers who produce what she called real food, not products made to look like food.
The Response Splits Experts
Reaction from scientists and nutrition leaders has been divided. Some, including former FDA commissioner Dr. David Kessler, praised the stronger push toward whole foods and called it a big step forward.
Others warned that putting red meat and saturated fat near the top ignores long-standing research tied to heart disease. Stanford nutrition researcher Christopher Gardner said he was disappointed to see red meat given such a high priority. He said it conflicts with a large body of evidence on cardiovascular risk.
As the event wrapped up, Kennedy held a 10-page guideline document. It’s much shorter than the 164-page report released in 2020. He said the shorter format is intentional.
He argued that the answer to the country’s health problems isn’t found in a new drug. He said it comes down to everyday food choices. He also said the age of the ultra-processed American diet needs to end, with a return to simpler basics.
Trending News:
Medicare Benefit Changes in 2026: 5 Major Updates to Costs, Part D, and Medicare Advantage

Medicare updates matter every year because small rule changes can raise your monthly bill, shift what you pay at the pharmacy, or change how much protection you have if you get sick. For 2026, the Medicare Benefit Changes are big enough that it’s worth a quick check, even if you’re happy with your plan today.
Most of the key updates start January 1, 2026, and they touch the areas people feel most: Part B costs, Part D drug spending, and Medicare Advantage limits. In this post, you’ll see the five biggest changes, who they affect, and what to do next before you re-enroll or stick with what you have.
For example, a retiree taking several brand-name prescriptions could see a very different year once the Part D out-of-pocket cap is in place, especially if they usually hit the catastrophic phase. A couple on Part B might also feel the premium and deductible increases right away. Keep in mind, costs and rules can still vary by plan and state, so the details matter.
Change in 2026 Part B costs: higher monthly premium and deductible
Medicare Part B is the part of Original Medicare that helps pay for doctor visits, outpatient care (like ER visits that don’t lead to an admission, imaging, labs, and same-day surgery), and many preventive services (like screenings and annual wellness visits). For 2026, Part B gets more expensive in two ways you feel right away: the monthly premium and the yearly deductible.
Here’s what changed:
| Part B cost | 2025 | 2026 | Change |
|---|---|---|---|
| Standard monthly premium | $185.00 | $202.90 | +$17.90 |
| Annual deductible | $257 | $283 | +$26 |
Most people have their Part B premium taken out of their Social Security check, so this update often shows up as a smaller monthly deposit, not a bill you pay manually.
To make it real, here’s quick math (not counting any coinsurance after the deductible):
- One person (standard premium): $202.90 × 12 = $2,434.80 per year in premiums, plus the $283 deductible, for $2,717.80 before most cost-sharing even begins. In 2025, that same “premium + deductible” baseline was $2,477.00. That’s $240.80 more in 2026.
- A couple (both on standard premium): premiums are $202.90 × 12 × 2 = $4,869.60, plus $283 × 2 = $566 in deductibles, for $5,435.60. In 2025, it was $4,954.00, which is $481.60 more in 2026.
For the official numbers, CMS posts the annual updates in its fact sheet: 2026 Medicare Parts A and B premiums and deductibles.
Who pays the standard premium vs income-based surcharges (IRMAA) in 2026
IRMAA stands for Income-Related Monthly Adjustment Amount. In plain English, it means higher earners pay more each month for Medicare Part B (and usually an add-on for Part D too).
Two details trip people up:
- IRMAA looks back at a prior tax year. For 2026 Medicare premiums, Social Security generally uses your 2024 tax return.
- Income thresholds can change each year. For 2026, the starting threshold is $109,000 for single filers (modified adjusted gross income, based on 2024 taxes). If you’re at or under that level, you typically pay the standard $202.90 Part B premium.
If your income crosses into IRMAA territory, your Part B premium can jump sharply. The frustrating part is that it may reflect a year that doesn’t match your life now, like your last working year or a year with a big one-time gain.
Simple ways to stay ahead of it:
- Review your last tax return: Look at your 2024 MAGI and see if you are close to the $109,000 (single) line.
- Plan for one-time income spikes: Selling a home, large IRA withdrawals, Roth conversions, and capital gains can push you into a higher bracket.
- Ask about an appeal if your income dropped: Retirement, reduced work hours, divorce, or the death of a spouse can qualify you for an IRMAA reconsideration through Social Security, so you’re not stuck paying a surcharge based on an old, higher-income year.
For a plain-English overview of how IRMAA works and why people get surprised by it, this summary is helpful: Medicare Premiums 2026: IRMAA brackets and surcharges for Parts B and D.
How to plan for Part B increases without skipping care
When Part B rises, it’s tempting to put off appointments. That often backfires. A better approach is to treat the premium like a utility bill, then protect the care that keeps you stable.
A few practical moves that help:
- Build the premium into your monthly budget: If your premium comes out of Social Security, adjust your spending plan for a smaller deposit. If you pay Medicare directly, set up an automatic payment so you don’t miss it.
- Check for help paying Medicare costs: Ask your state Medicaid office about Medicare Savings Programs, and ask Social Security about Extra Help for Part D drug costs. Even if you think you earn too much, it’s worth a quick check.
- Use preventive care that’s covered: Many preventive services under Part B are covered (often with $0 cost to you when requirements are met). Getting screenings and wellness visits on time can prevent expensive surprises later.
- Reduce billing surprises before they happen: Always confirm whether a provider accepts Medicare assignment. When they do, they agree to Medicare-approved amounts, which helps limit what you can be billed. If they don’t, your share can be higher, and the bills can feel like they came out of nowhere.
These Medicare Benefit Changes for 2026 are manageable with a plan, but they’re hard to absorb if you only notice them after your check hits the bank.
Change in 2026 Medicare Advantage spending cap: lower in-network out-of-pocket maximum
One of the most practical Medicare Benefit Changes for 2026 is a small but real improvement to your financial backstop in Medicare Advantage (Part C).
A Medicare Advantage plan has an annual out-of-pocket maximum for covered, in-network services under Medicare Part A and Part B. Once your spending on those covered services hits the limit, your plan covers eligible in-network Part A and Part B costs at 100% for the rest of the year (you still pay your monthly premium, and drug costs follow Part D rules).
For 2026, the maximum allowed in-network out-of-pocket cap is $9,250, down from $9,350 in 2025. Many plans set their cap lower than the limit, so your plan may offer better protection, but the national rule matters when plans reset benefits each year. For a primary source, see CMS: 2026 Medicare Advantage and Part D Advance Notice Fact Sheet.
Why the out-of-pocket max matters even if you feel healthy right now
It’s easy to focus on the monthly premium because it’s predictable. The out-of-pocket max is different; it’s there for the year your health takes a turn.
Picture this: you feel fine all year, then you slip on ice and need unexpected surgery. Suddenly, you have an ER visit, imaging, the surgeon, anesthesia, a hospital stay, follow-up specialist visits, and weeks of rehab therapy. Each step can bring a copay or coinsurance, and those smaller bills can add up fast.
That’s the key difference:
- Premiums: what you pay every month to keep the plan.
- Out-of-pocket costs: what you pay when you use care (copays, coinsurance, and sometimes deductibles).
Your plan’s out-of-pocket maximum is like a seat belt. You hope you never need it, but you want it to work when things go wrong. And the lower the cap, the less you risk paying in a bad health year.
A few important fine-print points:
- The cap applies to covered services, and usually only to in-network care (depending on plan design).
- Out-of-network rules can be different. Some plans have a higher combined limit, some cover less out of network, and some HMOs may not cover non-emergency out-of-network care at all.
- Extra benefits like dental, vision, and hearing often have their own limits (like a yearly dollar cap) and may not count toward the medical out-of-pocket maximum.
Questions to ask your plan for 2026: in-network, referrals, prior authorizations
Before you re-enroll, treat your plan like you’re checking the locks on your house. You’re not expecting trouble; you just want fewer surprises later.
Use this checklist when you review your 2026 materials or call the plan:
- Network check: Are my doctors, specialists, and preferred hospital in-network for 2026, not just today?
- Specialist costs: What is the copay or coinsurance for a specialist visit, and does it change after a certain number of visits?
- Outpatient procedures: What will I pay for common outpatient care like same-day surgery, endoscopy, or infusion therapy?
- Referrals: Do I need a referral to see a specialist, and what happens if I skip it?
- Prior authorization: Which services need approval in advance, including:
- Imaging like MRI, CT, and PET scans
- Skilled nursing facility care after a hospital stay
- Home health visits, therapy, or durable medical equipment
- How approvals work: How long do authorizations last, and what paperwork does my doctor need to submit?
During Open Enrollment, read your plan’s Annual Notice of Change (ANOC) line by line. If your network shrinks, prior authorization expands, or your out-of-pocket max rises (even if it stays under the $9,250 cap), it’s a sign to compare other Medicare Advantage options for 2026.
Change in 2026 Part D costs: base premium and deductible go up.
Medicare Part D is the part of Medicare that helps pay for prescription drugs. You can get it two ways: as a standalone Part D plan (often called a PDP) that pairs with Original Medicare, or as drug coverage built into many Medicare Advantage plans (MA-PDs). Either way, Part D is where many people feel Medicare Benefit Changes the fastest, because prices show up every time you refill.
For 2026, two national benchmarks move higher:
- The 2026 national base beneficiary premium is $38.99, up from $36.78 in 2025.
- The Part D deductible limit is $615, up from $590 in 2025.
These numbers matter, but they’re not your bill. Think of the base premium as a yardstick Medicare uses for pricing and calculations. Your actual premium depends on the plan you choose and where you live, and it can be higher or lower than $38.99.
If you want the source straight from CMS, see: 2026 Medicare Part D Bid Information and Part D Premium Stabilization Demonstration Parameters.
Why your Part D premium might change more than the national average
Part D plans aren’t one-size-fits-all. Each plan can set its own mix of costs and rules, including:
- Premiums: what you pay each month to keep coverage.
- Formularies: the plan’s list of covered drugs (and which tier each drug is on).
- Pharmacy networks: where you get the best price (preferred pharmacies) versus where you pay more.
So even if the national base premium only inches up, your plan might still jump. One common reason is that plan pricing can shift when the federal premium stabilization support changes. For 2026, the premium stabilization subsidy is smaller (to $10 per month from $15), which can leave more room for plans to raise premiums or reprice benefits.
The practical takeaway is simple: don’t assume last year’s “good plan” stays good. Every fall, take 30 minutes to:
- Re-shop plans during Medicare Open Enrollment.
- Check whether your exact drugs (dose and form) are still covered.
- Confirm your pharmacy is still “preferred”, not just “in-network”.
Simple ways to lower Part D costs in 2026 (before you hit the deductible)
Before your plan starts sharing costs, the deductible is where people feel the sting. A few small moves can trim what you pay early in the year.
Start with your prescriptions. Ask your doctor or pharmacist:
- Can I use a generic? Generics often land on lower tiers.
- Is there a therapeutic alternative? Same goal, different drug, sometimes a lower copay.
- Can I change the timing? If it’s safe, syncing refills can cut extra pharmacy trips.
Then focus on where and how you fill:
- Use preferred pharmacies when possible; the same drug can cost more at a standard pharmacy.
- Ask about 90-day supplies (many plans allow this for maintenance meds), which can lower the cost per month and reduce refill hassles.
If you use a brand-name drug with a high list price, check whether manufacturer assistance is available and allowed for your situation. (Eligibility rules vary, and it’s not an option for every drug, but it can be worth checking.)
Finally, if you switch plans, compare the total yearly cost, not just the premium. A low premium can hide higher copays, a higher deductible, or a weaker pharmacy network. The best plan is the one that costs you less across the whole year, not just on January’s bill.
Change in 2026 Part D out-of-pocket cap: a $2,100 yearly limit for covered drugs.s
One of the biggest Medicare Benefit Changes in 2026 is a clear limit on what you can be billed for covered Part D drugs. Starting in 2026, once you personally spend $2,100 out of pocket on Part D-covered prescriptions (through a standalone Part D plan or a Medicare Advantage plan with drug coverage), your cost for covered drugs drops to $0 for the rest of the calendar year.
This matters most if you take high-cost brand drugs or specialty meds, like treatments for cancer, rheumatoid arthritis, multiple sclerosis, Crohn’s disease, psoriasis, or other autoimmune conditions. If your pharmacy receipts tend to snowball by mid-year, this cap is meant to stop the bleeding and give you a real stopping point.
For a consumer-friendly overview of how the cap works and what it means for people with costly medications, the PAN Foundation explanation is helpful: Understanding the Medicare Part D cap.
What counts toward the $2,100 cap and what might not
Think of the $2,100 cap like a scoreboard that only tracks one kind of spending: what you pay for drugs your Part D plan covers. If the plan doesn’t cover it, or you buy it in a way that bypasses the plan, it may not move you closer to the cap.
In general, these costs do count toward the $2,100 limit:
- Your Part D deductible (if your plan has one).
- Copays and coinsurance you pay for covered prescriptions after the deductible.
- Costs for covered drugs filled through the plan’s normal process (meaning the pharmacy runs your Part D insurance and you pay your share at pickup).
These costs often do not count (or may not count) toward the cap:
- Your monthly Part D premium. Premiums are separate from the out-of-pocket cap.
- Drugs not on your plan’s formulary (the plan’s covered drug list).
- Cash purchases outside the plan, like using a discount card or choosing not to run the medication through your Part D coverage.
- Out-of-network pharmacy purchases (depending on plan rules, especially if it’s not an emergency fill).
- Certain medications that are usually paid under Part B instead of Part D (your doctor’s office can tell you how a drug is billed).
Before you count on the cap to protect you, confirm three basics with your plan:
- Is your exact drug covered (same dose and form)?
- Are there rules like prior approval or “try this first” steps?
- Is your pharmacy in-network, and is it a preferred pharmacy for the lowest price?
Getting these answers upfront can prevent the worst kind of surprise, paying full price for something you assumed would be tracked toward your $2,100 limit.
How to use the cap to avoid surprise bills throughout the year
The cap is powerful, but you get the most value when you plan your year like a road trip: you check fuel, map the stops, and keep an eye on the gauge. A little planning early can help you avoid panic spending later.
A simple month-by-month approach:
- Before January: List your prescriptions, doses, and preferred pharmacies. Ask your plan for a yearly cost estimate based on your meds. It’s often shown in plan tools, or you can call member services.
- January to March: Expect higher costs if you hit the deductible early. If possible, set aside money for these months so you’re not caught short.
- April to June: Track your running total. Your plan should track it too, but it helps to stay aware if you’re on expensive meds.
- July to September: If you’re getting close to $2,100, double-check that refills are being billed under Part D correctly and at an in-network pharmacy.
- October to December: Use Open Enrollment to compare next year’s options, because formularies and pharmacy networks can change.
To stay organized, keep it simple:
- Save your pharmacy receipts.
- Read your Explanation of Benefits (EOB) statements; they show what you paid and how your plan counted it.
- If something looks off, call the plan quickly. Fixing errors is easier when the fill is recent.
Also, use your pharmacist as a partner. Ask direct questions like:
- “Is there a lower-cost covered option in my plan?”
- “Is this being run through my Part D insurance today?”
- “Would a 90-day supply cost less overall?”
If your costs are still high early in the year, you may also be able to spread them out using the Medicare Prescription Payment Plan, which can help with cash flow even when the total yearly cap stays the same: What’s the Medicare Prescription Payment Plan?.
Change in 2026 mental health benefits in Medicare Advantage: cost-sharing must not be higher than Original Medicare.
Mental health care can be hard to start and easy to stop. For a lot of people, the reason is simple: the bill feels too steep. One of the Medicare Benefit Changes in 2026 is designed to cut that barrier.
In plain terms, Medicare Advantage plans cannot charge you more out of pocket for many behavioral health services than you would pay under Original Medicare. That includes common care like therapy, counseling, outpatient mental health visits, and substance use treatment. The goal is straightforward: if you’re in Medicare Advantage, your cost-sharing for these services should be equal to or better than what Original Medicare would require.
For CMS details, see: Contract Year 2026 policy and technical changes final rule fact sheet.
What this means for copays for therapy, counseling, and substance use treatment
Cost-sharing is the part you pay when you use care. It usually shows up in two forms:
- Copay: a flat dollar amount (example: $30 per therapy visit).
- Coinsurance: a percentage of the allowed cost (example: 20% of the visit charge).
Under Original Medicare, most outpatient mental health care is paid under Part B, which generally means you pay the Part B deductible first, then 20% coinsurance of the Medicare-approved amount for covered services. The 2026 rule pushes Medicare Advantage plans to cap your share at that level or lower for many behavioral health services.
Here are examples of services this change is meant to protect:
- Outpatient therapy and counseling, including visits with licensed therapists, psychologists, and clinical social workers
- Psychiatry visits for medication management
- Outpatient substance use treatment, including intensive outpatient programs, in many cases
- Opioid treatment programs, which can have special cost-sharing rules
Even with the new limit, your plan’s details still matter, because access problems can look like “coverage” on paper while feeling like a locked door in real life. Pay close attention to:
- Networks: Your cost is usually lowest only if the provider is in-network. Out-of-network coverage varies, and some plans may not cover it (except emergencies).
- Prior authorization: Some plans may require approval before certain levels of care start (like intensive outpatient or partial hospitalization).
- Visit rules: Medicare covers mental health care, but your plan can still have how-to-use rules, like needing a referral, using certain sites of care, or following step requirements.
A simple way to think about it is this: the 2026 change can lower the “price tag,” but you still want to confirm the store is open. Review your plan’s Evidence of Coverage for 2026 and verify that your therapist, counselor, or treatment center is in-network.
How to find mental health care that takes your coverage in 2026
Finding a provider can take a few tries, so it helps to use a repeatable process. Here’s a practical approach that works for many Medicare Advantage members:
- Call your plan’s member services and ask for the exact benefit for outpatient mental health visits (copay or coinsurance), plus any prior authorization rules.
- Search the plan’s provider directory for therapists, counselors, psychiatrists, and substance use programs near you.
- Call the provider’s office and confirm your exact plan, not just “Medicare.” Ask, “Do you take my Medicare Advantage plan (plan name) for 2026?”
- Ask about telehealth. Many providers can offer video visits, which can widen your options and shorten wait times.
If you hit long wait lists, these tips often help you get seen sooner:
- Ask to be added to a cancellations list
- Consider group therapy, which can be effective and easier to schedule
- Ask your primary care doctor for a referral, especially if the plan prefers referrals for specialists
If someone is in immediate danger or at risk of harm, call 911 or go to the nearest emergency room right away.
Conclusion
These five Medicare Benefit Changes for 2026 all point to one thing: your costs and protections can shift even if you keep the same coverage. Part B will cost more upfront, so check the new premium and deductible and adjust your monthly budget now.
Medicare Advantage gets a slightly lower in-network out-of-pocket max, but your real risk is a network change, so confirm your doctors and hospitals are still in for 2026. Part D pricing is moving too, so re-shop plans using your exact medication list, then compare total yearly cost, not just the premium.
The $2,100 Part D out-of-pocket cap is a hard stop for covered drugs, but only if your meds are on the formulary and you fill them the right way, so verify coverage and pharmacy status before January. Medicare Advantage mental health cost-sharing should be no worse than Original Medicare for many services, so review the copays, prior approval rules, and provider availability, then lock in care early if you can.
Next 7 days checklist
- Gather an up-to-date meds list (name, dose, pharmacy, refill timing).
- Confirm your key providers and preferred hospital will be in-network for 2026.
- Compare Part D or MA-PD options during enrollment windows using your meds list.
- Set a simple budget for the 2026 Part B premium, Part B deductible, and any Part D deductible.
Thanks for reading, and before you make changes, verify the details with Medicare, your plan, or a licensed advisor who can review your situation end-to-end.
Trending News:
New Voter ID Laws 2026: How Will They Affect the 2026 Midterms




Israeli Strike Kills Iran’s Navy Commander Alireza Tangsiri

New Cicada COVID Variant Emerges: What to Know About BA.3.2

DOJ Investigation of Former CIA Director John Brennan Deepens

Adam Schiff Told to ‘Resign’ After Whistleblower Claims, FBI Opens Investigation

Trump Issues Stark Warning to NATO After Iran War Snub

Greta Thunberg Under Fire Over Derogatory Trump Remarks

Senate Hearing on Fraud and Foreign Influence Turns Tense Over Minnesota Scandals

Russia Tells Iran Scale Back Hostilities Toward the United States

CNN Forced to Backtrack Its Reporting on Trump’s Iran Talks

Joe Rogan Slams Gavin Newsom for Mocking Nick Shirley

Thai Billionaire Charged With Lese Majeste Over Facebook Post
Russia Bans Facebook, Meta Says It’ll Do “Everything” To Restore Service

Facebook Login Feature – Clash of Clans

4 Things you can do to take your Facebook Lead Generation to the Next Level

Zuckerberg to Allow Violent Speech on Russia After Facebook Blocked

Facebook Loses $200 Billion as Users Shift to TikTok

Downloading Facebook Videos Anonymously with High Quality Video through Snapsave app

The Best Site to Buy Real Facebook Likes and Followers in 2022

Chinese Man Arrested for Using Facebook to Dupe Cryptocurrency Investor

Google and Facebook Under Huge Pressure Over User Privacy
Senate Hearing on Fraud and Foreign Influence Turns Tense Over Minnesota Scandals
CNN Forced to Backtrack Its Reporting on Trump’s Iran Talks
Joe Rogan Slams Gavin Newsom for Mocking Nick Shirley

Mosque Set Ablaze in Iran a Citizens Revolt Against the Islamic Regime

AOC Accuses Jessie Watters of Fox News of Sexualizing and Harassing Her

JD Vance Exposes Walz’s Fraud and CNN’s Lies in White House Presser

Milestone Card Credit: How the Milestone MasterCard Can Transform Credit
-

 China2 months ago
China2 months agoChina-Based Billionaire Singham Allegedly Funding America’s Radical Left
-

 Politics2 months ago
Politics2 months agoCNN Delivers Stark Reality Check to Democrats Over Voter ID
-

 Midterm Elections3 months ago
Midterm Elections3 months ago2026 Midterms Guide: Candidates, Key Issues, and Battleground States
-
 News3 months ago
News3 months agoMosque Set Ablaze in Iran a Citizens Revolt Against the Islamic Regime
-

 Politics3 months ago
Politics3 months agoIlhan Omar’s Finances Under Fire Amid Minnesota’s Massive Fraud Scandal
-

 Politics3 months ago
Politics3 months agoPressure Builds for Tim Walz to Resign After Viral Video of Somali Daycare Fraud
-

 Health3 months ago
Health3 months agoRFK Jr Introduces the New Food Pyramid to “Make America Healthy Again”
-

 News3 months ago
News3 months agoTurning Point USA Under Scrutiny Over Alleged Shady Dealings